Loculated Pleural Effusion On Ultrasound - Pleural effusions are characterized on ct by attenuation values between those of water (0 hounsfield units hu) and soft tissue (approximately 100 hu), typically in the order of 10 to 20 hu.
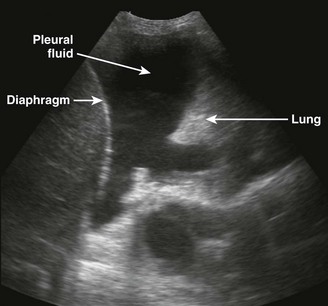
Loculated Pleural Effusion On Ultrasound - Pleural effusions are characterized on ct by attenuation values between those of water (0 hounsfield units hu) and soft tissue (approximately 100 hu), typically in the order of 10 to 20 hu.. Note the presence of a fibrin strands extending from the lung to the diaphragm, resulting in loculations of the pleural effusion. Loculated effusions are difficult to confirm with chest radiograph, but ultrasound, computed tomography (ct), and even magnetic resonance imaging (mri) may be used to verify a localized collection of pleural fluid. This is that small effusion labeled in he still image along with the moving image up on the right. The interpreting radiologists were blinded to the results of the chest ct and chest ultrasound when reviewing either study. 1 pleural effusion is defined as abnormal fluid collection in the pleural space.
A transudate is always anechoic in nature, while an exudate may show the following features: Most effusions start like this and can be easily missed. Approximately 1.5 million patients are diagnosed with pleural effusion each year in the united states. She was admitted to the hospital and a right sided 14 fr pigtail thoracotomy tube was placed. In contrast to the radiologic method, the ultrasonic technique permitted an easy differentiation between loculated pleural effusion and pleural thickening.
2 Lung Ultrasound Pre Reading For Fcus Course Intensive Care Network from intensivecarenetwork.com The pleural space is normally filled with ~5 to 10 ml of serous fluid, which is secreted mainly from the parietal pleura at a rate of 0.01 ml/kg/h and absorbed through the lymphatics. If needed, the fluid can be drained to make this distinction. Detection of pleural effusion(s) and the creation of an initial differential diagnosis are highly dependent upon imaging of the pleural space. This type of effusion is empyema unless proven otherwise. Pleural fluid is seen extending to the right oblique fissure. There is smooth pleural thickening with calcification and volume loss (rib crowding) on the right. Ultrasound can aid in the diagnosis of pleural effusion. Ultrasound of a loculated pleural effusion.
Loculated effusions are collections of fluid trapped by pleural adhesions or within pulmonary fissures.
Pleural effusions are characterized on ct by attenuation values between those of water (0 hounsfield units hu) and soft tissue (approximately 100 hu), typically in the order of 10 to 20 hu. This ultrasound was taken with a 3 mhz probe. However, in the setting of a massive pleural effusion and pneumonia with consolidation. Encysted pleural fluid is visualized between the right upper and middle lobe (s). Loculated effusions are difficult to confirm with chest radiograph, but ultrasound, computed tomography (ct), and even magnetic resonance imaging (mri) may be used to verify a localized collection of pleural fluid. This in turn helps to narrow down the differentials for the cause of effusion. Pleural effusion aspiration with ultrasound *. Based on the ultrasound features, it can also help to differentiate between a transudative and an exudative effusion. E7.8 loculated effusion loculated effusion. The largest pocket of fluid is present posteriorly at the right lung base, with associated atelectasis and minor consolidation. Pleural fluid is seen extending to the right oblique fissure. Prior chest radiographs indicating that the blunting is a new finding also provide a good indicator of pleural effusion. This type of effusion is empyema unless proven otherwise.
Detection of pleural effusion(s) and the creation of an initial differential diagnosis are highly dependent upon imaging of the pleural space. This ultrasound was taken with a 3 mhz probe. Pleural effusion aspiration with ultrasound *. A hemothorax on pulmonary ultrasound typically appears an effusion with a homogenous echogenic appearance. Based on the ultrasound features, it can also help to differentiate between a transudative and an exudative effusion.
Sonographic Evaluation Of Pleural Effusion from html.scirp.org Ultrasound is a valuable tool in difficult cases such as small pleural effusion or in loculated effusion. For the first time the superiority of the ultrasonic method over the radiologic one was demonstrated, and the difference was most obvious in cases of small pleural effusion. In contrast to the radiologic method, the ultrasonic technique permitted an easy differentiation between loculated pleural effusion and pleural thickening. 2 types generally are 1: Loculated effusions are difficult to confirm with chest radiograph, but ultrasound, computed tomography (ct), and even magnetic resonance imaging (mri) may be used to verify a localized collection of pleural fluid. However, in the setting of a massive pleural effusion and pneumonia with consolidation. This in turn helps to narrow down the differentials for the cause of effusion. Pleural effusion was defined as loculated if the collection had a lobulated or lenticular shape with a convex border 4, 5.
Most effusions start like this and can be easily missed.
A transudate is always anechoic in nature, while an exudate may show the following features: Thoracic ultrasound has become an increasingly valuable tool in the evaluation of critically ill patients in the emergency department (ed). The interpreting radiologists were blinded to the results of the chest ct and chest ultrasound when reviewing either study. The pleural space is normally filled with ~5 to 10 ml of serous fluid, which is secreted mainly from the parietal pleura at a rate of 0.01 ml/kg/h and absorbed through the lymphatics. Six patients with either malignant pleural effusion or empyema, in whom multiple conventional attempts at thoracocentesis were unsuccessful, were evaluated by ultrasound. However, in the setting of a massive pleural effusion and pneumonia with consolidation. Loculated effusions are difficult to confirm with chest radiograph, but ultrasound, computed tomography (ct), and even magnetic resonance imaging (mri) may be used to verify a localized collection of pleural fluid. The second effusion is loculated. Images were examined for the presence of pleural effusion and fibrin strands within the effusion. For the first time the superiority of the ultrasonic method over the radiologic one was demonstrated, and the difference was most obvious in cases of small pleural effusion. Note that the pigtail catheter in a is positioned below (rather than within) the loculated effusion, which explains why the catheter did drain any fluid until it was subsequently. Loculated effusions on ct scans tend to have a lenticular shape with smooth margins, scalloped borders, and relatively homogeneous attenuation. Based on the ultrasound features, it can also help to differentiate between a transudative and an exudative effusion.
We're not really seeing it anteriorly, but in the back you can again see that spine sign the very small triangular area of fluid with a little bit of lung waving around in it. For the first time the superiority of the ultrasonic method over the radiologic one was demonstrated, and the difference was most obvious in cases of small pleural effusion. A hemothorax on pulmonary ultrasound typically appears an effusion with a homogenous echogenic appearance. Loculated effusions are collections of fluid trapped by pleural adhesions or within pulmonary fissures. Pleural effusion was defined as loculated if the collection had a lobulated or lenticular shape with a convex border 4, 5.
Thoracentesis Clinical Gate from clinicalgate.com Conventional chest radiography and computed tomography (ct) scanning are the primary imaging modalities that are used for evaluation of all types of pleural disease, but ultrasound and magnetic resonance. A bedside ultrasound was then performed, showing a loculated pleural effusion (figure 2). In contrast to the radiologic method, the ultrasonic technique permitted an easy differentiation between loculated pleural effusion and pleural thickening. Prior chest radiographs indicating that the blunting is a new finding also provide a good indicator of pleural effusion. Radiological imaging of pleural diseases. E7.8 loculated effusion loculated effusion. Icu patients cannot sit up and the effusion layers posteriorly. The interpreting radiologists were blinded to the results of the chest ct and chest ultrasound when reviewing either study.
For the first time the superiority of the ultrasonic method over the radiologic one was demonstrated, and the difference was most obvious in cases of small pleural effusion.
Contrary to the radiological method, ultrasound allows an easy differentiation of loculated pleural fluid and thickened pleura. If needed, the fluid can be drained to make this distinction. There is smooth pleural thickening with calcification and volume loss (rib crowding) on the right. The long, thin white arrows indicate b lines, and the short, thick white arrow indicates the pleural margin. This is the shred or fractal sign. In contrast to the radiologic method, the ultrasonic technique permitted an easy differentiation between loculated pleural effusion and pleural thickening. On ct, the fluid collection is unchanged on coronal (b) and axial (c) images (arrows), proving that it is loculated. Approximately 1.5 million patients are diagnosed with pleural effusion each year in the united states. Pleural fluid studies are summarized in table 1. Most effusions start like this and can be easily missed. The pleural space is normally filled with ~5 to 10 ml of serous fluid, which is secreted mainly from the parietal pleura at a rate of 0.01 ml/kg/h and absorbed through the lymphatics. Note the presence of a fibrin strands extending from the lung to the diaphragm, resulting in loculations of the pleural effusion. The largest pocket of fluid is present posteriorly at the right lung base, with associated atelectasis and minor consolidation.
Contrary to the radiological method, ultrasound allows an easy differentiation of loculated pleural fluid and thickened pleura loculated pleural effusion. Pleural fluid studies are summarized in table 1.






0 Komentar